Hey thereif you've ever felt a stubborn lump in your neck or armpit and brushed it off as "just a swollen gland," you're not alone. A painless, slowly growing node can be easy to ignore, but for some people it's the first whisper of lymphocyterich Hodgkin's lymphoma (LRHL), a rare slice of the broader Hodgkin's lymphoma family. Below you'll get straighttothepoint answers: what LRHL actually is, how it shows up, how doctors pin it down, and what the most effective treatments look like today. Let's dive in togetherno fluff, just the info you need.
What Is LRHL?
Definition & Classification
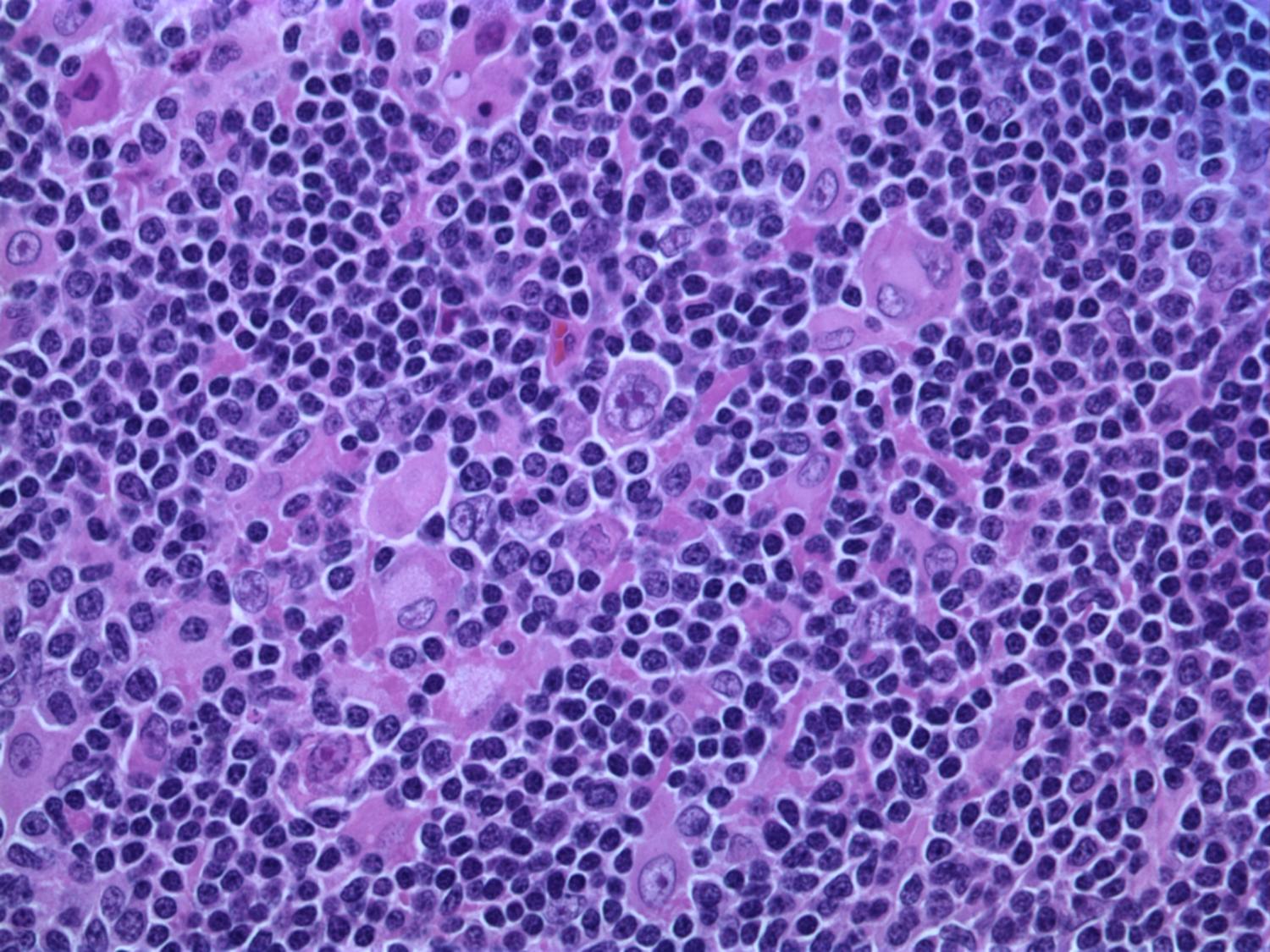
LRHL is asubtype of classical Hodgkin lymphoma (CHL). While CHL accounts for about 10% of all lymphomas, LRHL makes up only ~5% of those cases. Pathologically, you'll see classic ReedSternberg cellsthose large, "owleyes" appearing cellsnestled in a sea of small, seemingly ordinary lymphocytes. That background of tiny lymphocytes is what gives the subtype its name.
How It Differs From Other Hodgkin Types
Compared with the more common nodularsclerosis or mixedcellularity variants, LRHL tends to involve fewer bulky mediastinal masses and shows a lower rate of Bsymptoms (fever, night sweats, weight loss). In other words, it often feels less "aggressive" on imaging, even though it's still a form of lymphatic system cancer that needs prompt attention.
| Feature | LRHL | Other CHL Subtypes |
|---|---|---|
| Background cells | Numerous small lymphocytes | Mixed inflammatory cells (eosinophils, neutrophils) |
| Typical stage at diagnosis | StageIII (early) | Often StageIIIIV |
| Common Bsymptoms | Rare (~10%) | More frequent (3040%) |
| Median age | 43years | 3035years |
Expert Insight
Hematopathology specialists often stress the importance of immunophenotypingchecking for CD15, CD30, and sometimes CD20to confirm the diagnosis. As one senior pathologist put it, "Seeing those ReedSternberg cells in a lymphocyterich field is like spotting a rare bird among a flock of sparrows."
Who Gets LRHL?
Epidemiology & Risk Factors
The typical LRHL patient is a man in his earlytomid40s, although women can be affected too (roughly a 2:1 maletofemale ratio). A handful of risk factors have shown up in studies:
- Prior infection with EpsteinBarr virus (EBV) the same virus that causes mononucleosis.
- Family history of Hodgkin lymphoma.
- Immunosuppression, such as HIV infection or posttransplant medication.
Data Snapshot
According to the SEER database, LRHL accounts for about 5% of all CHL diagnoses in the United States, with an incidence that has remained steady over the past two decades. A recent analysis in American Society of Hematology notes that EBV positivity is detected in roughly onethird of LRHL cases.
Signs & Symptoms
Core Clues You Can Feel
Think of the most common clue as a painless swollen lymph node. It's often found in the neck, underarm (axilla), or groin and may feel like a rubbery bean that doesn't hurt when you press on it. Many patients also report an "allover fatigue" that feels heavier than normal tiredness.
BSymptoms Not the Main Story
Fever, night sweats, and unexplained weight loss are called Bsymptoms. In LRHL they're relatively rareonly about 10% of patients experience themso don't be fooled into thinking you're safe just because you don't have a fever.
When It Mimics Something Else
Because swollen nodes can also come from infections, reactive inflammation, or even a harmless cyst, it's easy to misattribute the lump. That's why a definitive tissue diagnosis is crucial; skipping a biopsy can delay the right treatment.
Quick Check List
- New, painless node lasting >4weeks?
- Feeling unusually exhausted?
- Any night sweats or fever?
- Did the node change size after a cold?
If you answered "yes" to the first two, it's worth talking to a doctorpreferably one who knows the nuances of Hodgkin's lymphoma.
How Is LRHL Diagnosed?
Clinical Workup
The journey usually starts with a careful history (how long the node's been there, any accompanying symptoms) and a physical exam that maps out all palpable areasneck, armpits, groin, even the behindtheknees region.
Imaging & Lab Tests
A PETCT scan is the gold standard for staging. It lights up metabolically active tissue, letting doctors see if the disease is confined to one area or has spread. A standard CT can add detail about the size and exact location of nodes.
Blood work (CBC, ESR, liver and kidney panels) helps assess overall health and flags any hint of bonemarrow involvement.
Biopsy The Definitive Step
For LRHL, an excisional lymphnode biopsy is preferred over a fineneedle aspiration because it provides enough tissue to examine architecture and perform immunohistochemistry. Pathologists look for ReedSternberg cells surrounded by a rich lymphocyte background and apply stains for CD15, CD30, and sometimes CD20. EBVencoded RNA (EBER) testing can also be done.
Staging & Prognosis
Most patients present at StageI or II, meaning the disease is limited to one or two regions. Using the AnnArbor system, doctors assign an "A" or "B" suffix based on the presence of Bsymptoms. According to the NCCN guidelines, earlystage LRHL enjoys a slightly better progressionfree survival than some other CHL subtypes.
Diagnostic Flowchart
- History & physical exam
- Imaging (PETCT, CT)
- Laboratory studies
- Excisional biopsy pathology + immunophenotyping
- Staging (AnnArbor) treatment plan
Treatment Options
FirstLine Chemotherapy
The backbone of treatment is the ABVD regimen (Adriamycin, Bleomycin, Vinblastine, Dacarbazine). For earlystage LRHL, ABVD alone yields a complete remission (CR) rate of about 95%.
Radiation Therapy
When a bulky node remains after chemotherapy, an involvedsite radiation therapy (ISRT) is added. This targeted approach spares healthy tissue while delivering a "final sweep" to any lingering cancer cells.
Targeted & Immunotherapy
For relapsed or refractory disease, newer agents have changed the game:
- PD1 inhibitors (pembrolizumab, nivolumab) block a checkpoint that cancer cells use to hide from the immune system. Studies show an overall response rate (ORR) around 80% in Hodgkin lymphoma, including LRHL.
- Brentuximab vedotin targets CD30 on ReedSternberg cells, delivering a cytotoxic payload directly to the tumor.
StemCell Transplant
If the disease is chemorefractory, an autologous stemcell transplant can provide a second chance at longterm remission. It's an intensive procedure, but for many it offers a realistic path to cure.
Comparison of Key Regimens
| Regimen | Typical Stage | CR Rate | Main SideEffects |
|---|---|---|---|
| ABVD | III | 95% | Neutropenia, lung toxicity (Bleomycin) |
| ABVD+ISRT | III (bulky) | 97% | Radiation dermatitis, fatigue |
| PD1 inhibitor (ABVD) | Relapsed | 80% ORR | Immunerelated AEs (colitis, pneumonitis) |
| Brentuximab vedotin | Relapsed/ refractory | 70% ORR | Peripheral neuropathy, fatigue |
Expert Quote
Dr.Linda Chen, a leading hematologistoncologist, notes, "For most earlystage LRHL patients, ABVDISRT remains the gold standard, but the availability of PD1 blockade gives us a powerful safety net when the disease returns."
Managing Side Effects & Supportive Care
Common Chemotherapy Toxicities
ABVD can make you feel nauseous, cause hair loss, and lower blood counts, raising infection risk. Staying hydrated, eating small frequent meals, and using prescribed antiemetics can make a world of difference.
LongTerm Considerations
Because many LRHL patients are diagnosed in their 40s, thinking ahead about fertility, heart health, and secondary cancers is essential. A cardiopulmonary evaluation before starting Bleomycin and regular followup screenings (echocardiograms, pulmonary function tests) are standard practice.
Lifestyle Tips for Recovery
- Proteinrich meals to help rebuild tissue (think lean meats, beans, tofu).
- Gentle walks or yoga to maintain stamina without overexertion.
- Prioritize sleepaim for 79hours each night.
- Stay connected with support groups; sharing experiences reduces isolation.
Resources
You're not alone. Organizations like the Lymphoma Research Foundation, MyLymphomaTeam, and local cancer support groups offer free counseling, patienttopatient mentorship, and practical guides (downloadable nodepalpation charts, treatment timelines, etc.).
Getting Help & Trusted Information
Professional Guidelines
Both the NCCN guidelines and the American Society of Clinical Oncology (ASCO) provide evidencebased recommendations for Hodgkin lymphoma, including LRHL. These resources are updated annually and reflect consensus from top experts.
PatientFocused Websites
Sites such as the Lymphoma Research Foundation and MyLymphomaTeam host realworld stories from people who've walked the same path. Reading a survivor's journey can demystify the medical jargon and give you a sense of hope.
What to Ask Your Doctor
When you sit down with your oncologist, consider these questions:
- What stage is my disease, and what does that mean for treatment?
- Are there clinical trials for LRHL that might be appropriate for me?
- How will we monitor for longterm side effects?
- What support services are available at my treatment center?
Building Trust
Good doctors welcome these questions and will provide clear, jargonfree answers. If you ever feel something is unclear, don't hesitate to ask for clarification or a second opinionthat's part of taking charge of your health.
Conclusion
Even though lymphocyterich Hodgkin's lymphoma is a rare form of lymphatic system cancer, the outlook is overwhelmingly positive when it's caught early and treated with the modern arsenal of chemotherapy, targeted radiation, and immunotherapy. Recognizing those painless swollen nodes and persistent fatigue can be the first step toward a cure. Remember, you don't have to navigate this alonelean on trusted medical guidelines, connect with patient communities, and keep an open dialogue with your care team. If you have questions or want to share your own experience, drop a comment belowwe're all in this together.
FAQs
What are the most common early signs of lymphocyte‑rich Hodgkin's lymphoma?
The disease usually begins with a painless, rubbery swelling in the neck, armpit, or groin. Fatigue is also frequently reported, while classic B‑symptoms (fever, night sweats, weight loss) are rare in early stages.
How is lymphocyte‑rich Hodgkin's lymphoma definitively diagnosed?
A definitive diagnosis requires an excisional lymph‑node biopsy. Pathologists look for Reed‑Sternberg cells in a background of many small lymphocytes and confirm with immunohistochemistry (CD15, CD30, often CD20) and EBV testing.
What imaging studies are used to stage the disease?
PET‑CT is the gold‑standard for staging because it highlights metabolically active tissue and detects spread. A conventional CT scan can provide additional anatomic detail.
What is the standard first‑line treatment for early‑stage LRHL?
Most patients receive the ABVD chemotherapy regimen (adriamycin, bleomycin, vinblastine, dacarbazine). When a bulky node remains after chemo, involved‑site radiation therapy (ISRT) is added.
Which newer therapies are available for relapsed or refractory LRHL?
PD‑1 inhibitors (pembrolizumab, nivolumab) and brentuximab vedotin have shown high response rates in relapsed disease. Autologous stem‑cell transplant is an option for chemorefractory cases.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a healthcare professional before starting any new treatment regimen.
Related Coverage

Fatigue, unexplained fevers, and swollen lymph nodes were early signals that led to my lymphoma diagnosis. Learning these subtle symptoms helped me catch it at an early, treatable stage....

DLBCL treatment guide covers R‑CHOP, Pola‑R‑CHP, CAR‑T, precision drugs, and clinical trial options for better outcomes....

Lymphocyte‑rich Hodgkin's lymphoma often presents as painless swollen nodes; learn its symptoms, diagnosis steps, and treatments....

Lymphocyte-depleted Hodgkin's lymphoma presents with swollen nodes, fever, night sweats, progression; learn signs and treatment....

Find key signs, stages, and current treatments for Hodgkin lymphoma, plus survival rates and advice for talking with your doctor....

Mixed cellularity Hodgkin's lymphoma signs, diagnosis, treatment options, and prognosis explained clearly for patients and families....

Effective treatments for recurrent Hodgkin lymphoma include high‑dose chemo, stem‑cell transplant, targeted drugs, and trials....

Learn about Sjögren's lymphoma risk, who’s most vulnerable, early warning signs, and how monitoring helps you stay proactive....

Take this quick lymphoma symptoms quiz to help assess your risk and determine if lingering issues like swollen nodes, fever, fatigue and weight loss warrant seeing a doctor....
Practical guide on diffuse large B‑cell lymphoma: symptoms, diagnosis, staging, treatment options, and post‑therapy follow‑up....